Delirium – Avoid using antipsychotics if QTc is prolonged
If the patient has an indication for antipsychotics (due to behavior that is a danger to self or others or distressing psychosis) but the use in contraindicated due to a prolonged QTc, there are limited options.
This is a optimal time to revisit and emphasize the nonpharmacologic standard interventions.
Restraints are often used but remember they can prolong and worsen severity of delirium and are associated with serious injury or death. “Restraints should only be used as a last resort, in the least-restrictive manner, and for the shortest time possible” (American Geriatrics Society – Choosing Wisely)
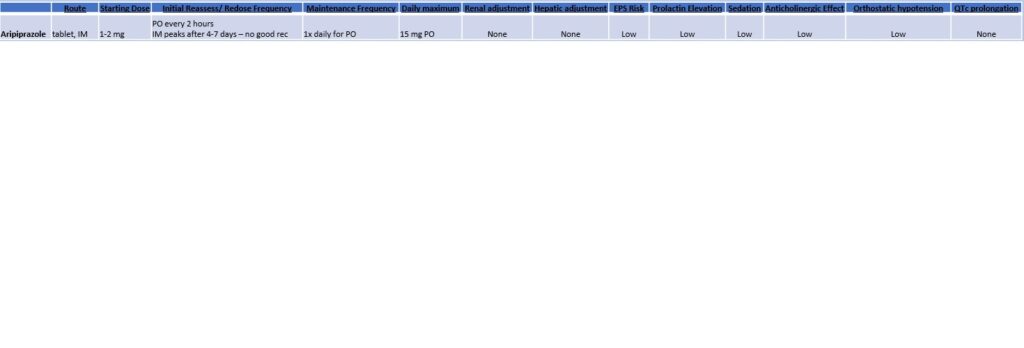
Aripiprazole is a hypothetically attractive antipsychotic choice because it may have the lowest risk of QTc prolongation and has a more favorable side effect profile. However, it has not been as rigorously studied an other antipsychotics in delirium and its use is complicated by a long half life. The long half life creates difficulty in potentially reaching a steady state, redosing the medication, and there is no clear guidance on non-oral formulations which may be needed in a patient unable to take oral.
In our experience, it may be reasonable to use aripiprazole as it tends to be well tolerated but is of questionable efficacy
- Alternatively, you could consider low dose benzodiazepines understanding that it will probably prolong and worsen the delirium
Finally, keep rechecking the EKG while treating reversible causes of QTc prolongation