UTI: Localizing Signs and Symptoms
Pearl: Symptoms such as change in cognition, agitation/aggression, decreased appetite, nausea +/- vomiting, syncope and falls are NOT symptoms of UTI in older adults in the absence of genitourinary tract specific signs and symptoms.
Localizing signs or symptoms (must be NEW or WORSENING)
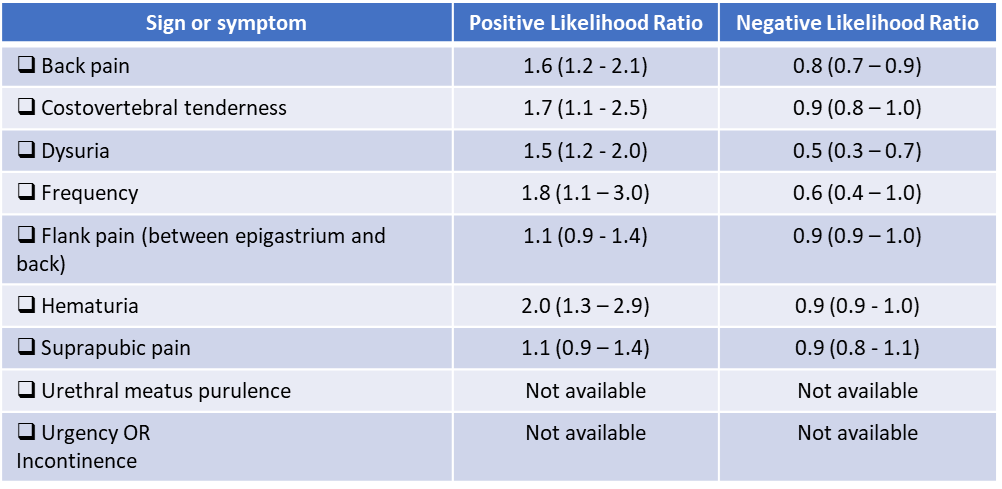
This data is extrapolated to older adults who, by definition, have “complicated” UTIs and to men. While not ideal, there is sparse data on the signs and symptoms of urinary tract infections in older adults.
Quick note on UTI diagnostic criteria:
There is no universally accepted diagnostic criteria and most recommendations are on expert consensus. As previously discussed, the diagnosis of UTI is difficult in older adults for a variety reasons. Any rigid diagnostic algorithm is likely over or under diagnose cases. For example:
- Surveillance criteria for long term care facilities (McGeer and NHSN) were retrospectively designed to compare UTI cases.
- These criteria are NOT recommended to be routinely used for diagnosing and treating UTIs.
- Other consensus criteria (Loeb minimum criteria, AHRQ, and decision tools) have been developed but all have limitations.
- Loeb: If fever and dysuria are absent, having urgency, rigors/chills, incontinence, and would not meet minimum criteria
- Both surveillance and Loeb (and likely other strict criteria) may underdiagnose compared to experts as the gold standard
What is NOT a sign or symptom of a UTI?
- “Dark, cloudy, or foul-smelling urine is not sufficient to indicate a UTI and may instead reflect mild dehydration or changes to diet or medications” (JAMDA consensus – Diagnosis of UTI)
- “Nonspecific symptoms — including change in cognition, agitation [or aggression], decreased appetite, [nausea +/- vomiting, syncope] and falls – are not symptoms of UTI, especially when genitourinary tract specific signs and symptoms are absent” (JAMDA consensus – Role of Behavioral Change; emphasis added)
In older patients with functional and/or cognitive impairments with bacteriuria and without local genitourinary symptoms or other signs of infection (fever, hemodynamic instability) who experience delirium or a fall, we recommend assessment for other causes and careful observation rather than antimicrobial treatment.” IDSA Asymptomatic Bacteriuria Guidelines 2019 – Recommendations V1 and V2 - Vaginal discharge or irritation makes a UTI unlikely (Does This Woman Have an Acute Uncomplicated Urinary Tract Infection)
A quick word on behavioral change in older adults with dementia.
- There is limited evidence to support behavioral change as evidence of a UTI.
- Because of the high prevalence of asymptomatic bacteriuria, there is a high likelihood that urine cultures collected will be positive regardless of the resident’s mental status at any given time
- In a resident with clear cut delirium, a UTI should only be considered if there is no other cause. Current recommendations suggest that there should be systemic (fever, chills, leukocytosis) or specific urinary findings to attribute a UTI as the cause of delirium
- In older adults with a change in mental status, the diagnosis of UTI is a diagnosis of exclusion
- Source: JAMDA Consensus Guidelines 2020 – Role of Behavioral Change of a Resident in diagnosing a UTI
What about constitutional signs or symptoms?
Fever, rigors, malaise, lethargy, loss of functional status are all constitutional signs or symptoms. They may be attributable to the urinary tract if no other etiologies are found after comprehensive evaluation.