Delirium – Work up for unclear etiology
Pearls:
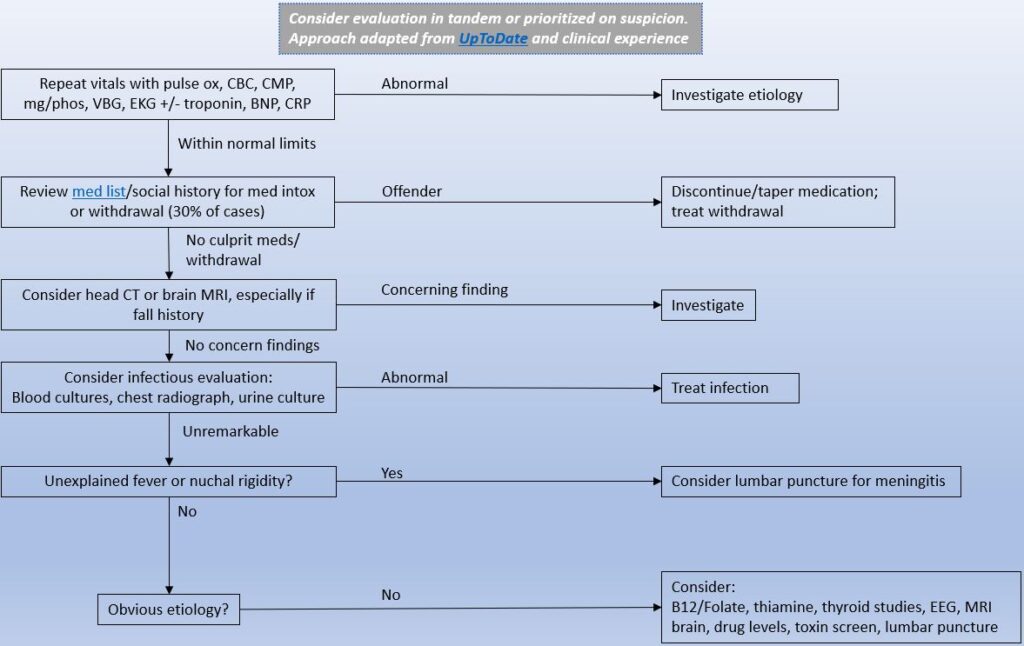
In the absence of fever/leukocytosis, hemodynamic, and localizing urinary symptoms, delirium is not a sign of UTI and other etiologies should be evaluated. Any bacteriuria should be viewed as asymptomatic and not subject to antibiotics per the Infectious Disease Society of America (IDSA) and Journal for Post-Acute and Long-Term Care (JAMDA).
- “Nonspecific symptoms — including change in cognition, agitation, decreased appetite, and falls – are not symptoms of UTI, especially when genitourinary tract specific signs and symptoms are absent” (JAMDA – Role of Behavioral Change)
- In older patients with functional and/or cognitive impairments with bacteriuria and without local genitourinary symptoms or other signs of infection (fever, hemodynamic instability) who experience delirium or a fall, we recommend assessment for other causes and careful observation rather than antimicrobial treatment.” IDSA Asymptomatic Bacteriuria Guidelines 2019 – Recommendations V1 and V2
Head imaging is not recommended in the initial evaluation unless there are neurologic deficits or recent head trauma (such as due to a fall).
- Utility of Head CT Scan for Acute Inpatient Delirium – Hospital Topics (2015)
- Diagnostic yield of head computed tomography for the hospitalized medical patient with delirium – Journal of Hospital Medicine (2014)
The role of B12/Folate, thiamine, thyroid studies, EEG, MRI, drug levels, toxin screen, and lumbar puncture in the initial evaluation of a patient with delirium is very limited unless there is high clinical suspicion.